
Denial Management in Medical Billing: Stop Losing Revenue You’ve Already Earned
| Quick Answer Denial management in medical billing is the systematic process of identifying, correcting, appealing, and preventing denied insurance claims. Effective denial management has two phases: reactive (fixing and resubmitting denied claims) and proactive (analyzing root causes to prevent the same denials from recurring). RevGen Billing’s denial management uses RPA-driven root-cause analysis to reduce denial rates and recover revenue from claims that would otherwise be written off. |
Why Claim Denials Are Costing You More Than You Think
There’s a number that most practice managers never calculate: the total annual revenue written off not because the claims couldn’t be paid, but because nobody followed up in time. In the practices I’ve audited, it’s rarely the result of coding errors. It’s the result of denials that aged past timely filing limits because the denial management workflow didn’t exist.
A claim denial isn’t a rejection it’s a decision by the payer not to pay based on specific criteria. That decision is often reversible with the right documentation, the right appeal, filed within the right window. The problem is that window closes. And once it closes, that revenue is gone.
Systematic denial management makes sure nothing ages past that window. Every denied claim gets reviewed, categorized, corrected, and resubmitted or appealed before the clock runs out.
What Are the Most Common Reasons Claims Get Denied?
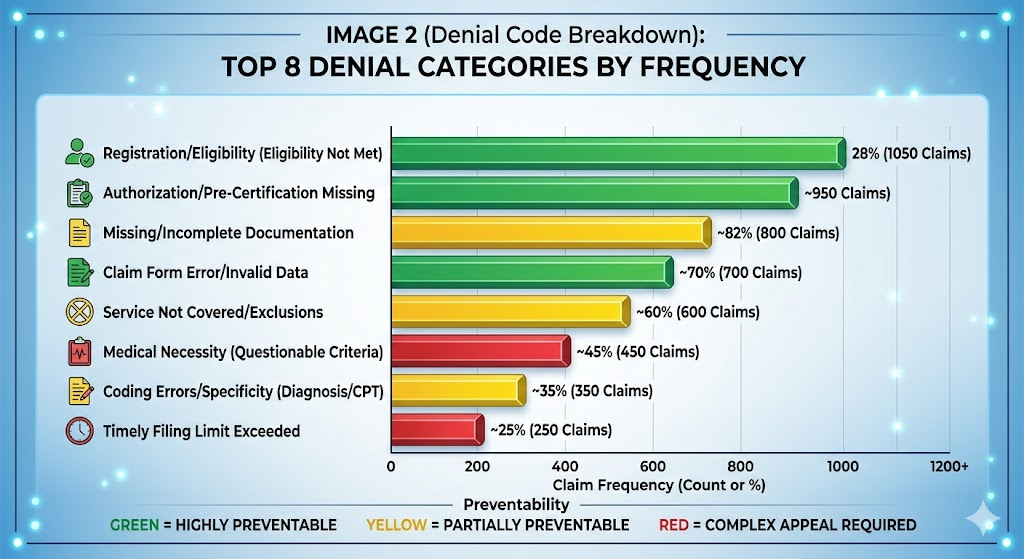
| Denial Category | Common Cause | Prevention Strategy |
| Eligibility/Coverage | Insurance lapsed or plan doesn’t cover service | Real-time eligibility verification pre-visit |
| Authorization Missing | Prior auth not obtained before procedure | Authorization tracking and alerts before scheduling |
| Coding Errors | Wrong CPT, ICD-10 mismatch, missing modifier | Certified coder review before submission |
| Timely Filing | Claim submitted past payer deadline | Claims submitted within 24–48 hours of service |
| Duplicate Claim | Same claim submitted twice | RPA duplicate detection before submission |
| Credentialing Gap | Provider not enrolled with payer | Proactive credentialing renewal tracking |
| Medical Necessity | Documentation doesn’t support billed diagnosis | Pre-submission clinical documentation review |
| Coordination of Benefits | Primary/secondary payer order incorrect | COB verification during eligibility check |
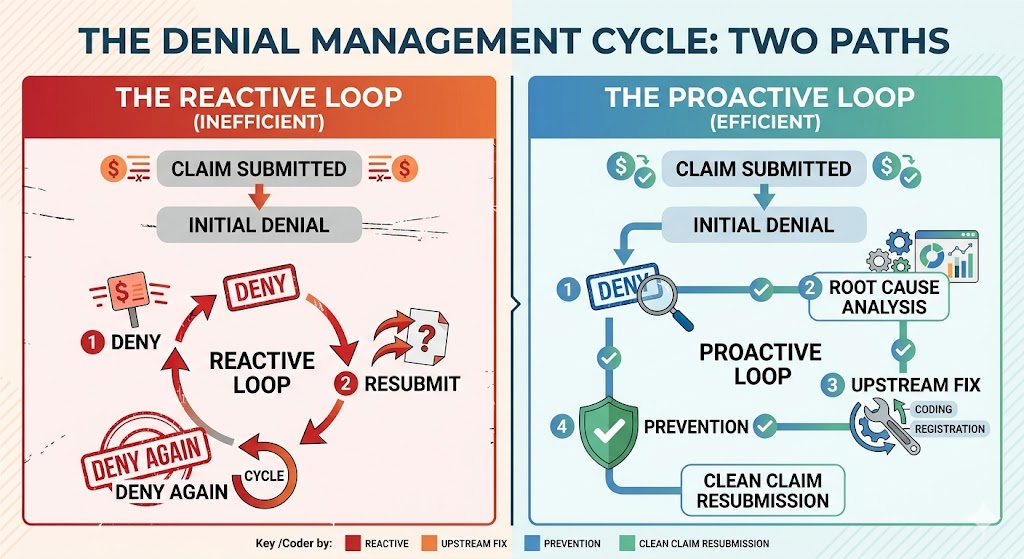
What Is the Difference Between Reactive and Proactive Denial Management?
Reactive Denial Management
Most billing companies operate reactively. A claim gets denied, someone looks at the denial code, corrects the obvious error, and resubmits. This approach doesn’t reduce your denial rate it just processes the same denials month after month, indefinitely.
Proactive Denial Management
Proactive denial management tracks denial patterns across payers, procedure codes, and providers. If CO-4 (modifier missing) denials are clustering around a specific CPT code with a specific payer, that’s a systemic problem not a one-off error. RevGen’s denial management workflow identifies those patterns and corrects the upstream process, so the denial stops recurring.
This is the difference between treating symptoms and treating the disease. Reactive management keeps you busy. Proactive management reduces your workload over time.
| Billing Community Observation A frequently recurring question in medical billing forums: ‘We’re resubmitting denied claims but our denial rate isn’t improving what are we doing wrong?’ The answer is almost always the same: resubmission is not denial management. Real denial management requires categorizing every denial by root cause, tracking frequency by payer and code, and feeding that analysis back into the submission workflow. Without that feedback loop, you’ll resubmit the same denials forever. |
How Does RevGen’s Denial Management Process Work?

- Denial Capture — Every denied claim is flagged and categorized automatically using denial code classification.
- Root Cause Analysis — RevGen identifies whether the denial is a coding issue, eligibility problem, authorization gap, credentialing lapse, or documentation deficiency.
- Corrective Action — The appropriate correction is made: claim edit and resubmission, appeal with supporting documentation, or credentialing follow-up.
- Timely Filing Monitoring — All denials are tracked against payer-specific timely filing windows. Nothing ages past the appeal deadline.
- Trend Reporting — Monthly denial trend reports show your practice which denial categories are decreasing and which need further upstream correction.
- Prevention Loop — Denial data feeds back into the submission workflow, modifying pre-submission checks to prevent the same denial category from recurring.
| Find out which claim categories are your biggest denial risk. Free Denial Audit → revgenbilling.com/contact |
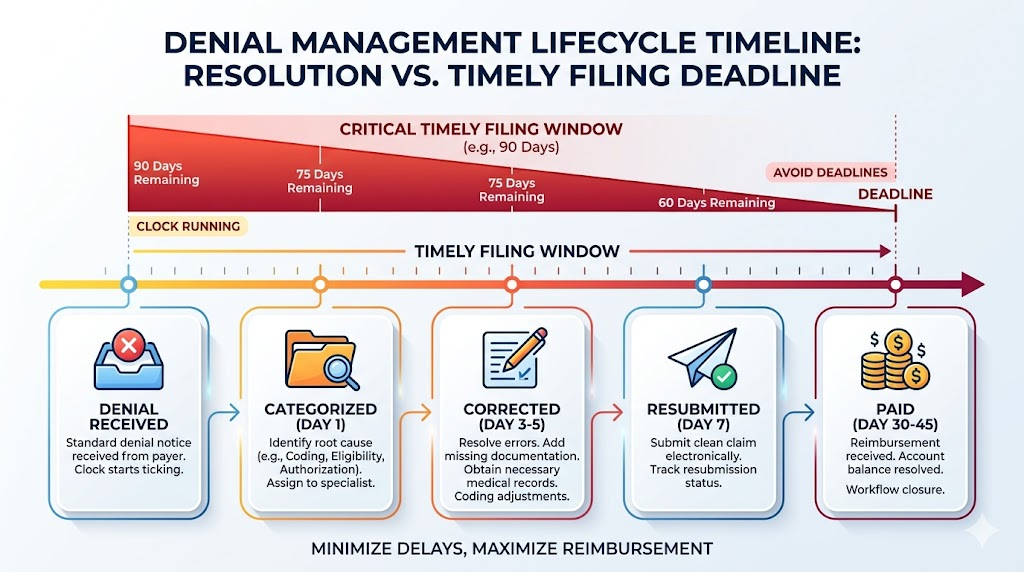
How Long Does It Take to Recover Revenue From Denied Claims?
Simple denials with clean corrections wrong modifier, missing authorization that can be obtained retroactively are typically resubmitted and paid within 30–45 days. Complex medical necessity denials requiring peer-to-peer review or full appeal can take 60–120 days depending on payer.
The most important variable isn’t the payer’s speed it’s how quickly the denial is worked. A denial that sits for 45 days before anyone looks at it has 45 fewer days in its appeal window. RevGen’s workflow assigns and works every denial within its first week.
Frequently Asked Questions
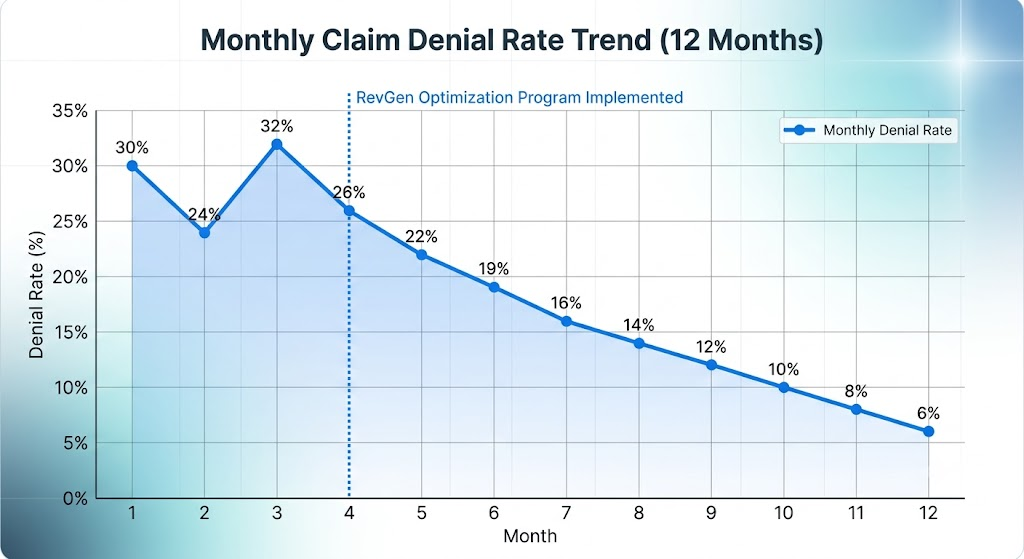
What is the denial rate for medical billing and what’s considered good?
The average claim denial rate across the healthcare industry ranges from 5% to 10% of submitted claims. A denial rate below 5% is considered strong. RevGen’s proactive denial management and 98% first-pass clean claim rate work together to keep denial rates well below industry average. Specialty matters surgical billing typically sees higher denial rates than primary care, requiring more specialized coding oversight.
What happens if a denial goes past the timely filing limit?
Once a claim exceeds the payer’s timely filing limit typically 90 to 365 days depending on the payer it becomes non-appealable and must be written off. This is one of the most preventable forms of revenue loss in medical billing. RevGen’s denial management workflow tracks all open denials against their respective timely filing windows to ensure no claim ages past its appeal deadline.
Can previously written-off denials be recovered?
In some cases, yes through waiver requests, corrected claim submissions to secondary payers, or patient billing for the outstanding balance. RevGen reviews historical AR for recovery opportunities during the free audit. Not every written-off claim can be recovered, but practices are often surprised by how much residual revenue exists in their aged AR.
What is a CO-4 denial code and how is it fixed?
CO-4 means the claim was denied because the procedure code is inconsistent with the modifier. This most commonly happens when modifier -25 is applied to a visit without a clearly documented separately identifiable E&M service, or when modifier -59 is used incorrectly. The fix requires reviewing the clinical documentation, correcting the coding and modifier application, and resubmitting with a clear narrative if required by the payer.
Does RevGen handle appeals as well as resubmissions?
Yes. Resubmissions (corrected claims) and formal appeals (dispute letters with supporting documentation) are both part of RevGen’s denial management workflow. For medical necessity denials, RevGen coordinates peer-to-peer review requests and prepares appeal documentation including clinical rationale and payer-specific supporting criteria.
How does denial management differ by specialty?
Surgical billing sees higher denial rates than primary care because of modifier complexity, prior authorization requirements, and bundling edits. Behavioral health billing faces different challenges authorization limits, session limits, and medical necessity documentation requirements. RevGen assigns denial management specialists with experience in the specific denial patterns common to each specialty.
Author Bio
Written by James R., Denial Management Specialist | James has spent over a decade specializing in claim denial prevention and appeals for physician practices and hospital-based billing departments. He’s built denial management workflows from scratch for practices that were writing off 15%+ of submitted claims and rebuilt them to sub-5% denial rates through root-cause analysis and upstream process correction. He writes for RevGen Billing on denial prevention strategy, payer-specific appeal tactics, and billing compliance.